

Abstract
Background: There is limited data comparing the outcomes of the two most common (FM or FB) RIC regimens in AML. Previous smaller retrospective studies suggest increased non-relapse mortality (NRM) but decreased relapse with FM based RIC with a variable effect on overall survival as compared to FB.
Methods: AML patients aged ≥18 years who had their 1st allo HCT using FM or FB (iv Bu only) RIC between 2001-2015 who had data reported to CIBMTR were studied. Patients with cord blood or identical twin donors, TBI as a part of conditioning, GVHD prophylaxis with T cell depletion/CD34 selection or post HCT Cyclophosphamide were excluded. Primary endpoint was overall survival (OS), and secondary endpoints included non-relapse mortality (NRM), relapse, leukemia free survival (LFS) and acute and chronic GVHD. Cox proportional hazards multivariable regression was used to compare the two RIC regimens while adjusting for significant patient, disease and transplant related factors. Major subgroup analysis included patients in CR pre-HCT.
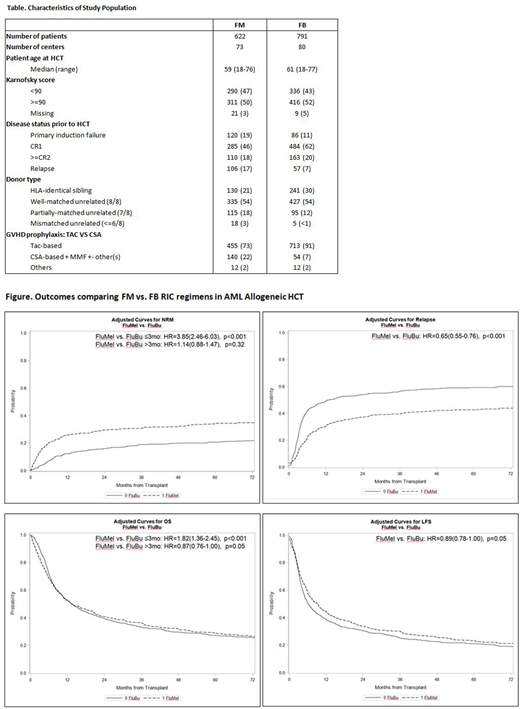
Results: 622 patients received FB and 791 had FM RIC. Median age of the FM group was 59 years, range (18 to 76) and median age of FB group was 61 years, range (18- 77). Compared to FB RIC regimen, FM group had more patients with active disease (36% vs 18%), with mismatched donors (24% vs 15%), with bone marrow grafts (19% vs 9%), HCT before 2005 (29% vs 12%) and without ATG/alemtuzumab (58 % vs 48%); but fewer patients in CR1 (46% vs 62%) and matched sibling donor grafts (21% vs 30%). There was significantly increased NRM in the FM vs FB within 3 mo post HCT (hazard ratio (HR)=3.85 (95% confidence intervals [CI] 2.46-6.03), but not beyond 3 mo FM vs FB , HR= 1.14 (95% CI 0.88-1.47). There was significantly decreased relapse for FM vs FB, (HR=0.65 (0.55-0.76), p<0.001) and a marginally superior LFS for FM vs FB, (HR=0.89 (95% CI 0.78-1.00), p=0.05). There was a lower OS FM vs FB within 3 mo post HCT (HR=1.82 (95% CI 1.36-2.45), p<0.001) but similar OS for FM vs FB beyond 3 mo post HCT (HR=0.87 (95% CI 0.76-1.00), p=0.05). Analysis restricted to only patients in CR pre-HCT showed similar results: equivalent survival, higher early NRM and lower relapse with FM.
Conclusion: The current study of this large CIBMTR AML transplant cohort has showed that in these two most common RIC regimens for allogeneic HCT, long-term survival with FM was similar to FB. While the FM regimen showed higher early NRM, it was associated with lower risks of relapse. Further analysis to evaluate FB and FM regimens in relationship to comorbidities, comprehensive geriatric assessments, and presence of minimal residual disease is warranted to better define the relative efficacy of these two RIC regimens in AML.
Weisdorf:Pharmacyclics: Consultancy; Seattle Genetics: Consultancy; SL Behring: Consultancy; FATE: Consultancy; Equillium: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal